

Abstract
Background: Plasma levels of imatinib have been shown to be predictive of disease response in chronic phase chronic myeloid leukemia (CML). However, the ultimate site of action of imatinib is intracellular. While intracellular imatinib has been reported to be correlated with plasma imatinib, the use of intracellular imatinib for the prediction of clinical outcomes is unclear. The concentration of intracellular imatinib depends on many factors including the level of alpha-1-acid glycoprotein, which binds to imatinib and prevents intracellular uptake, and the OCT-1 transporter, which mediates the influx of imatinib across the plasma membrane of leukemic cells. We conducted the present study of newly diagnosed CML patients with the primary objective of determining if intracellular levels of imatinib two weeks after treatment initiation predicted major molecular response. The secondary objectives were to elucidate the relationships between the levels of OCT-1 and plasma imatinib with intracellular imatinib.
Methods: We prospectively studied newly diagnosed chronic phase CML patients in Canada who were treated with standard dose imatinib (400 mg). We measured both intracellular and extracellular (plasma) levels of imatinib by tandem mass spectrometry at two weeks, four weeks, and twelve months after enrollment. Additionally, we measured transcript levels of OCT-1 and BCR-Abl by q-rt-PCR before treatment, at six months, and at twelve months to determine therapeutic response.
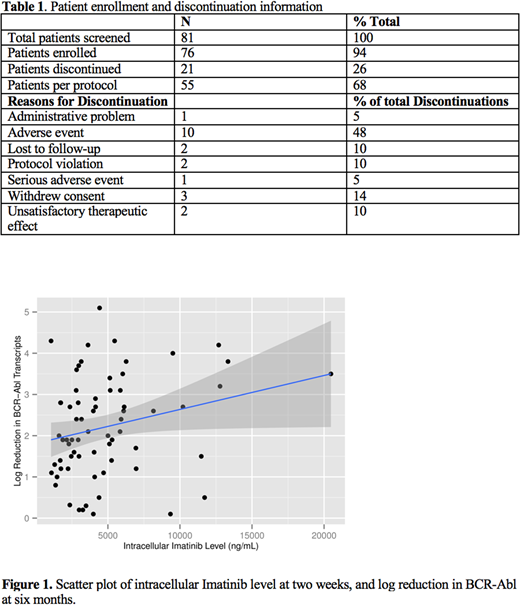
Results: Eighty-one patients were screened. A total of 76 patients entered the study, and 55 completed the study per protocol. Patient information is shown in Table 1. There was a significant correlation between intracellular imatinib levels at two weeks and a 2-log reduction of BCR-Abl transcript at six months (r=0.390; 95% CI = 0.136 - 0.595; p = 0.004) (Figure 1), but not at twelve months (r=0.183; 95% CI = -0.094 - 0.434; p = 0.194). Notably, intracellular imatinib levels and plasma levels of imatinib were highly correlated at two weeks (r=0.698; 95% CI = 0.559-0.799; p <0.001) and four weeks (0.699; 95% CI = 0.555 - 0.802; p < 0.001) but not between four weeks and twelve months (r= 0.230; 95% CI = -0.040 - 0.469; p = 0.094). There was no correlation between intracellular imatinib levels at two weeks and the pre-treatment OCT-1 transcript level (r=0.072; 95% CI = -0.166 to 0.301; p =0.556).
Conclusions: Intracellular imatinib levels at two weeks was moderately predictive of a disease response at six months as indicated by a 2-log reduction in BCR-Abl transcript. OCT-1 transcript levels did not have utility for predicting intracellular imatinib levels. Measurement of intracellular Imatinib levels may prove to have utility in identifying patients who would benefit from adjustments to therapy.
Hillis:Bristol-Myers Squibb: Honoraria; Novartis: Honoraria. Busque:Novartis: Consultancy; Pfizer: Consultancy; Paladin: Consultancy; BMS: Consultancy. Lipton:Bristol-Myers Squibb: Consultancy, Research Funding; ARIAD: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding. Savoie:Pfizer: Consultancy; Novartis: Consultancy, Honoraria; BMS: Consultancy, Honoraria. Leber:Novartis Canada: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis Canada: Honoraria, Membership on an entity's Board of Directors or advisory committees.

